
Published on July 2, 2025 9:35 PM GMT
Over the last two years or so, my girlfriend identified her cycle as having a unusually strong and very predictable effect on her mood/affect. We tried a bunch of interventions (food, sleep, socializing, supplements, reading the sequences, …) and while some seemed to help a bit, none worked reliably. Then, suddenly, something kind of crazy actually worked: Hair loss pills.
The Menstrual Cycle
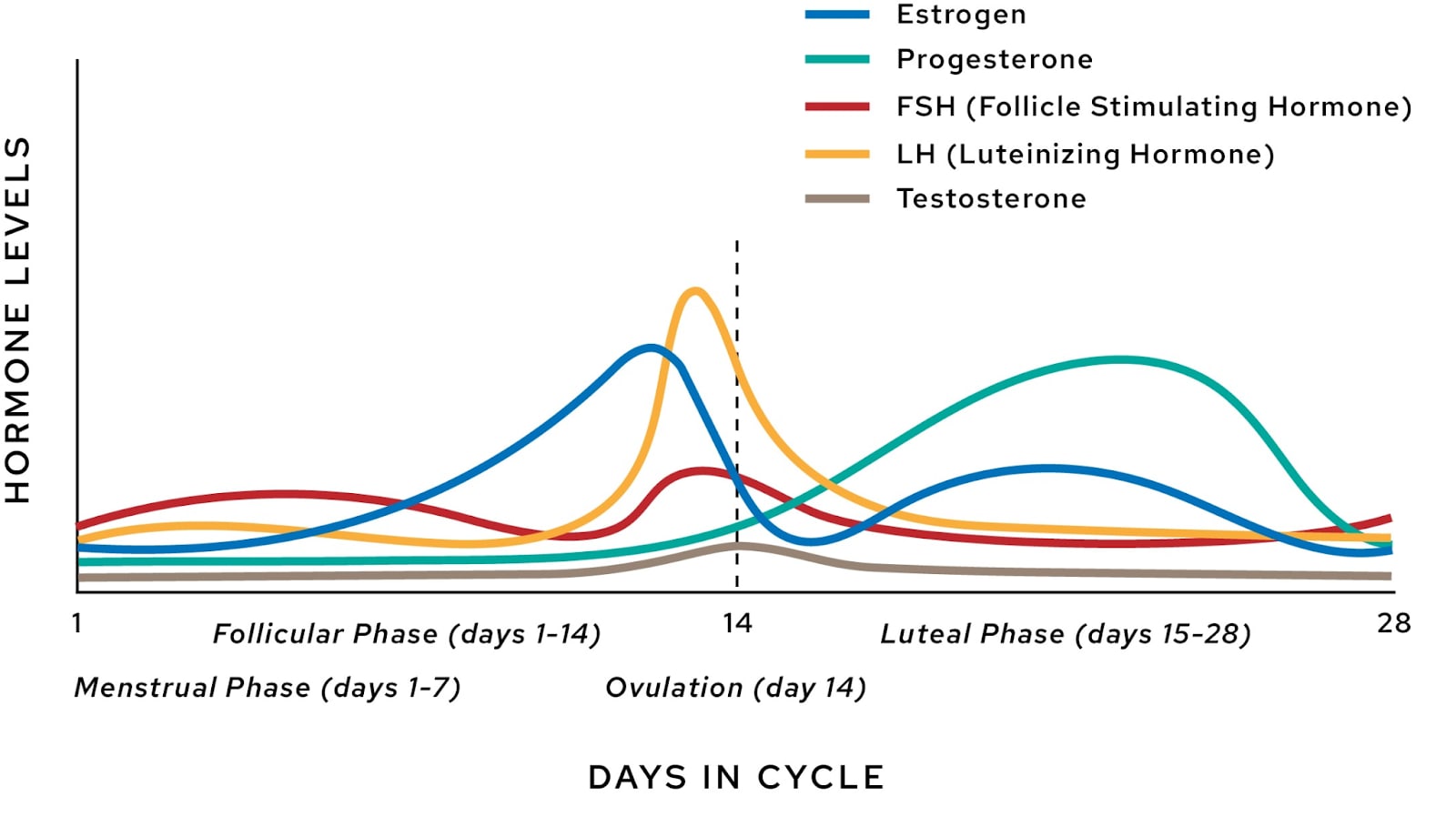
Quick review: The womenfolk among us go through a cycle of varying hormone levels over the course of about a month. The first two weeks are called the “Follicular Phase”, and the last two weeks are called the “Luteal Phase.” The first week (usually less) is the “period” (“menstrual phase”, “menses”) where the body sloughs off the endometrial lining in the uterus, no longer of use to the unimpregnated womb, and ejects it in an irregular fountain of blood and gore. After that is a steady ramp up of estrogen while the next egg matures by the end of the second week. Around that time, the egg is signaled to release by a spike in luteinizing hormone (LH) and this is called “ovulation”.
And then it all goes terribly, terribly, wrong.
The luteal phase is when women tend to experience PMDD (Premenstrual Dysphoric Disorder) / PME (Premenstrual Exacerbation,)[1] and at the end of the cycle, PMS (Premenstrual Syndrome). These look pretty similar from the outside (irritability, anxiety, sadness, etc,) but work through somewhat different though related mechanisms. (Probably. There is not, afaict, medical consensus on this.)
To understand why this happens, let’s zoom in to the second half of that hormone diagram from earlier:
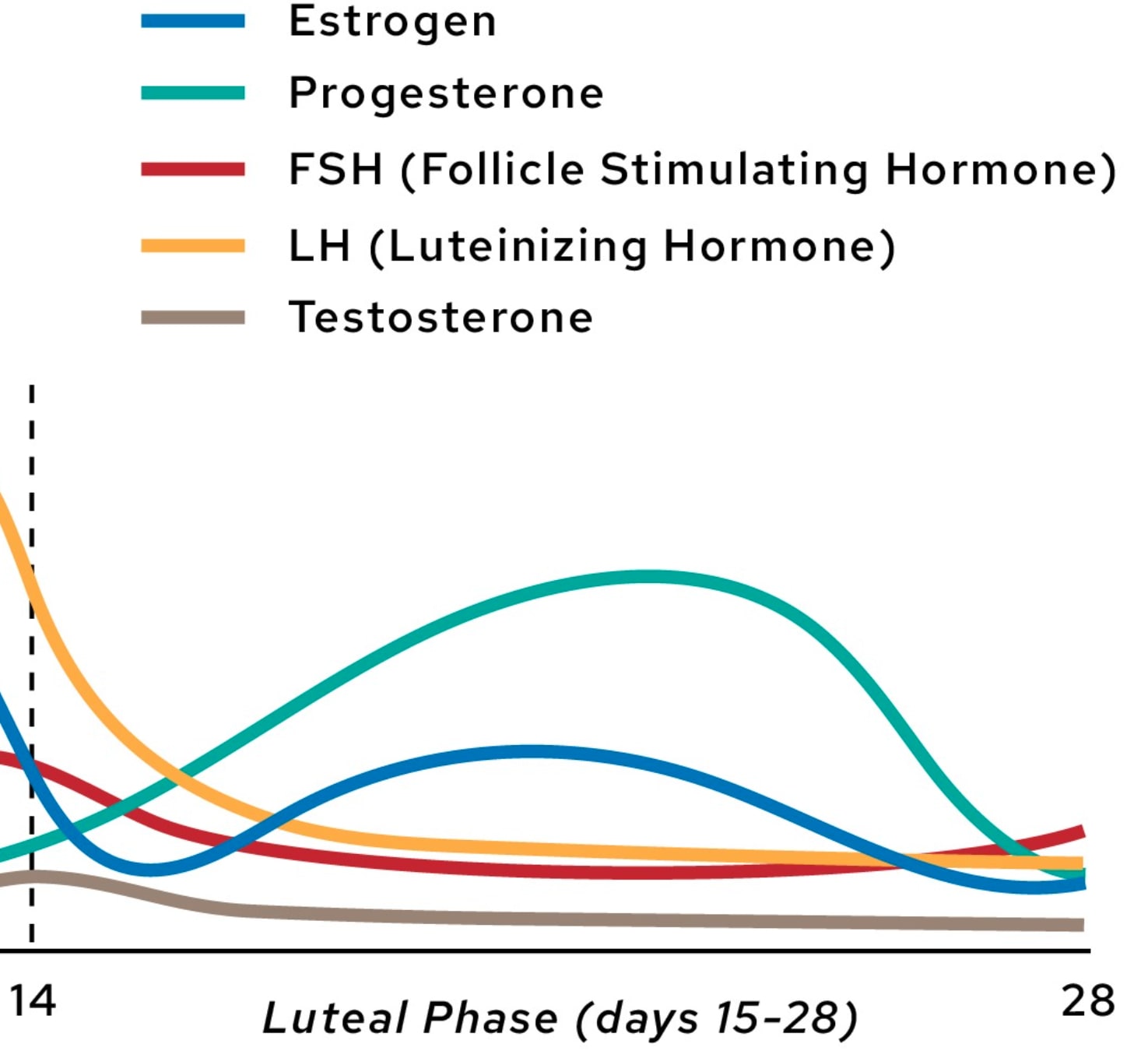
LH and FSH drop to steady levels for most of the luteal phase, while estrogen and progesterone ramp steadily upward. I submit progesterone as the relevant thing to track here.[2]
The Bad Guy: Progesterone Allopregnanolone
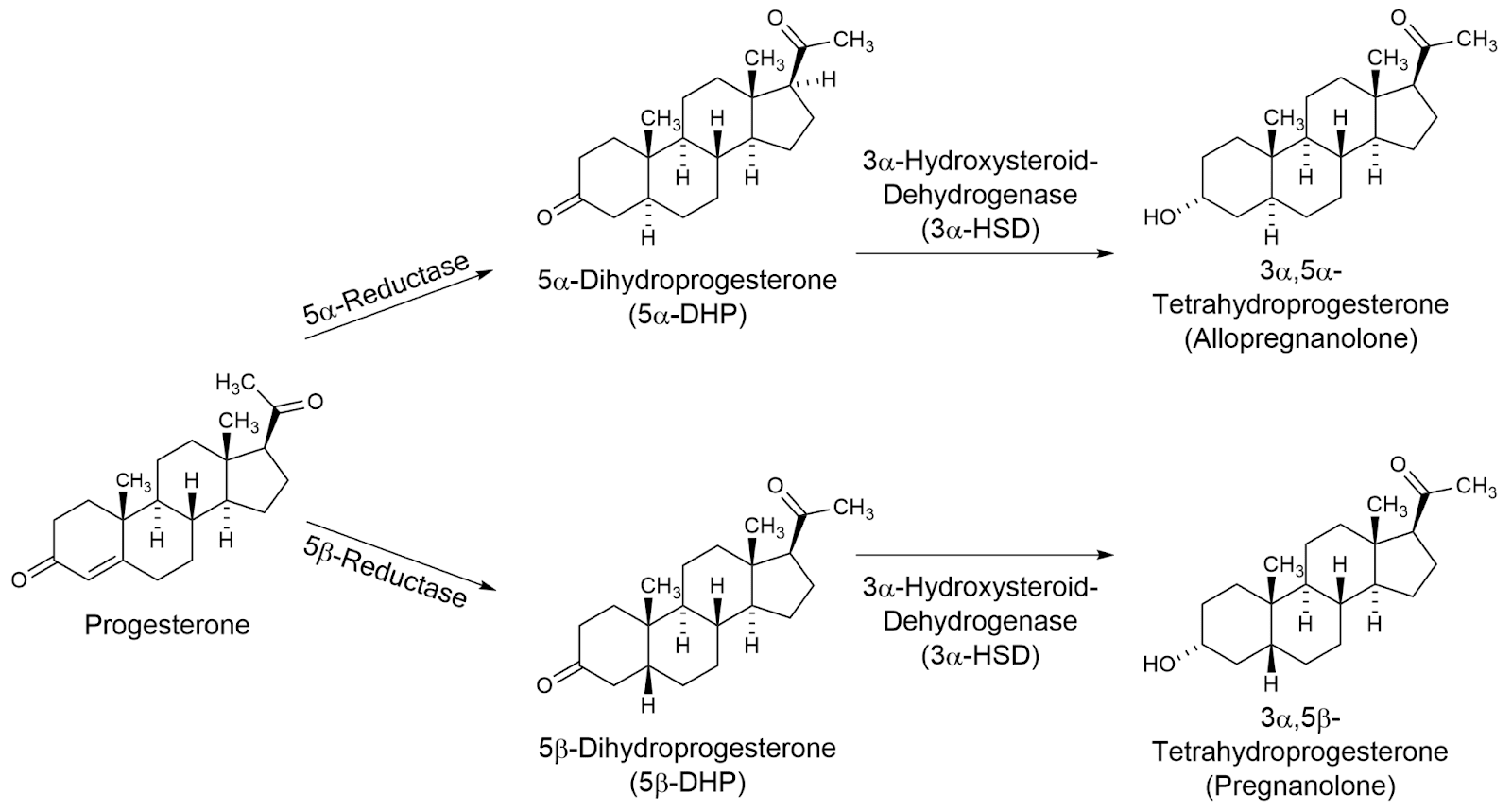
Progesterone is metabolized into a handful of different molecules, but the real villain is allopregnanolone (ALLO).
ALLO is a positive allosteric modulator of receptors, which means that in the presence of ALLO, receptors respond more strongly or more frequently to all the molecules that usually activate them. You know what else is a positive allosteric modulator of ? Xanax. And benzodiazepines in general.
The upshot is that, throughout the two weeks of the luteal phase, the concentration of ALLO floating around gets higher as progesterone levels rise, the brain develops some tolerance to the potentiated , until near the end when progesterone (and with it, ALLO) drops suddenly resulting in something like a minor form of benzo-withdrawal, a.k.a. PMS.
This explains that terrible spike in depression/anxiety/irritability/etc at the end of the cycle, and it explains the lethargy and brain-fog throughout the luteal phase, but not the PMDD throughout the luteal phase. In fact, if we are thinking of ALLO like Xanax, then in many ways it should be doing the opposite of PMDD during the luteal phase.
Luckily this model might survive by invocation of my least favorite thing in medicine: “paradoxical” reactions. These are when a particular drug/molecule known to have some specific effect has, in some people, in some circumstances, ~exactly the opposite effect. I don’t really understand what is going on when this happens, it seems like it’s very particular to each instance, but with ALLO it at least seems to be a known phenomenon.[3] (?) Does this mean that if I fed my girlfriend Xanax she would become more anxious/depressed/irritable rather than less? I haven’t tried it yet, but I’m very unsure what causes “paradoxical” reactions in the first place and so am pretty unsure how to generalize the apparent paradoxical effect of ALLO.
So now the full story of Luteal Hell: Ovulation hits and passes, and the body begins ramping up progesterone. In lock-step, ALLO levels rise and produce (in most women) lethargy and brain fog and (in some women, paradoxically) anxiety/depression/irritability/etc. That’s PMDD. Then, at the end of the luteal phase, the progesterone goes away and the ALLO with it, but the receptors have become accustomed to the benzo-like effects and so withdrawal hits as the receptors readjust. And that’s PMS.
Now, how do we fix it?
Hair Loss Pills
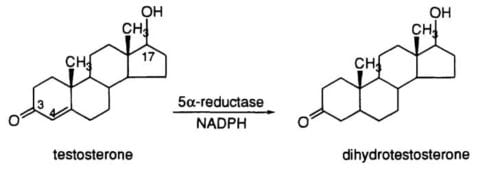
Enter, male pattern baldness. As I understand it, the Bad Guy of this story is DHT. DHT is metabolized from testosterone via an enzyme called 5α-reductase (5-AR), and among other things induces hair follicles to shrink (making individual hairs thinner and more brittle), reduces the anagen (growing) phase of the follicles (making the maximum hair length shorter), and increases shedding during the resting phase (causing the hair to fall out more quickly.) Thus, there are two main treatments for male pattern baldness which actually work:
The first is minoxidil (Rogaine) which seems to work by somehow lengthening the anagen (growing) phase of hair follicles in direct opposition to DHT which definitely helps, and also somehow widening the vessels/capillaries to increase blood flow to the follicles which…probably helps?
The second, is to attack the DHT problem directly, using drugs like finasteride or dutasteride that block DHT synthesis by binding-to and disabling the 5α-reductase enzyme.
…And that completes the list of effective hair-loss treatments! Minoxidil and 5-AR inhibitors.[4] But, hold on, haven’t we seen that guy before? Ah, there he is:
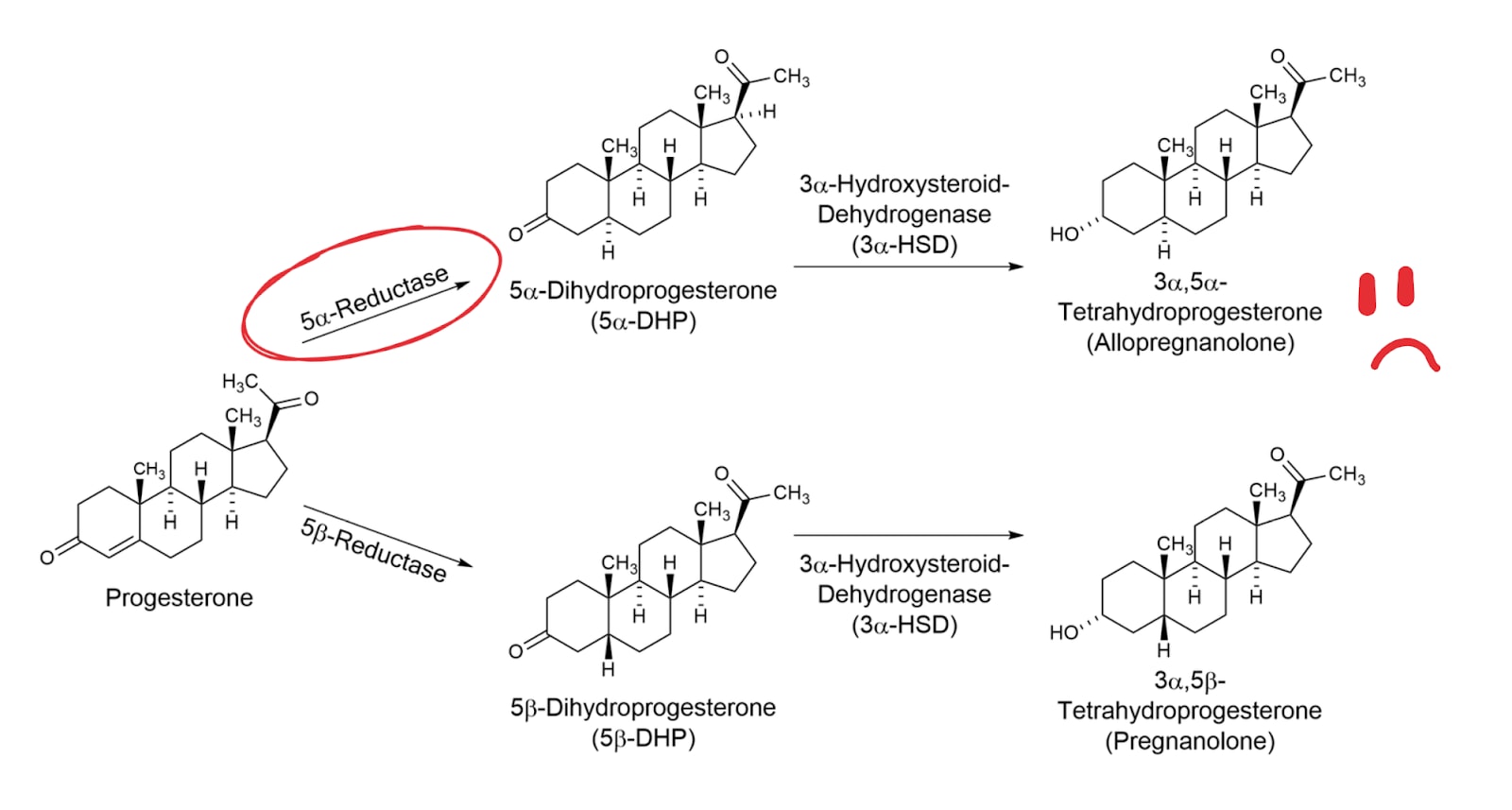
As it turns out, it just so happens that the very same enzyme which produces DHT from testosterone is also the first link in the chain from progesterone to ALLO! Now that’s a very helpful coincidence.[5]
So let’s take a look at our easily available PMS/PMDD-cure contenders.
Finasteride
This is the most commonly prescribed one of the two in the US. It’s often prescribed at 1mg for hair loss, sometimes 2.5mg and up to 5mg if you push for it which is the level used to treat enlarged prostates / prostate cancer. At around 1mg the serum levels of DHT seem to level off (at about 30% of un-inhibited) so more than that doesn’t do much of anything.
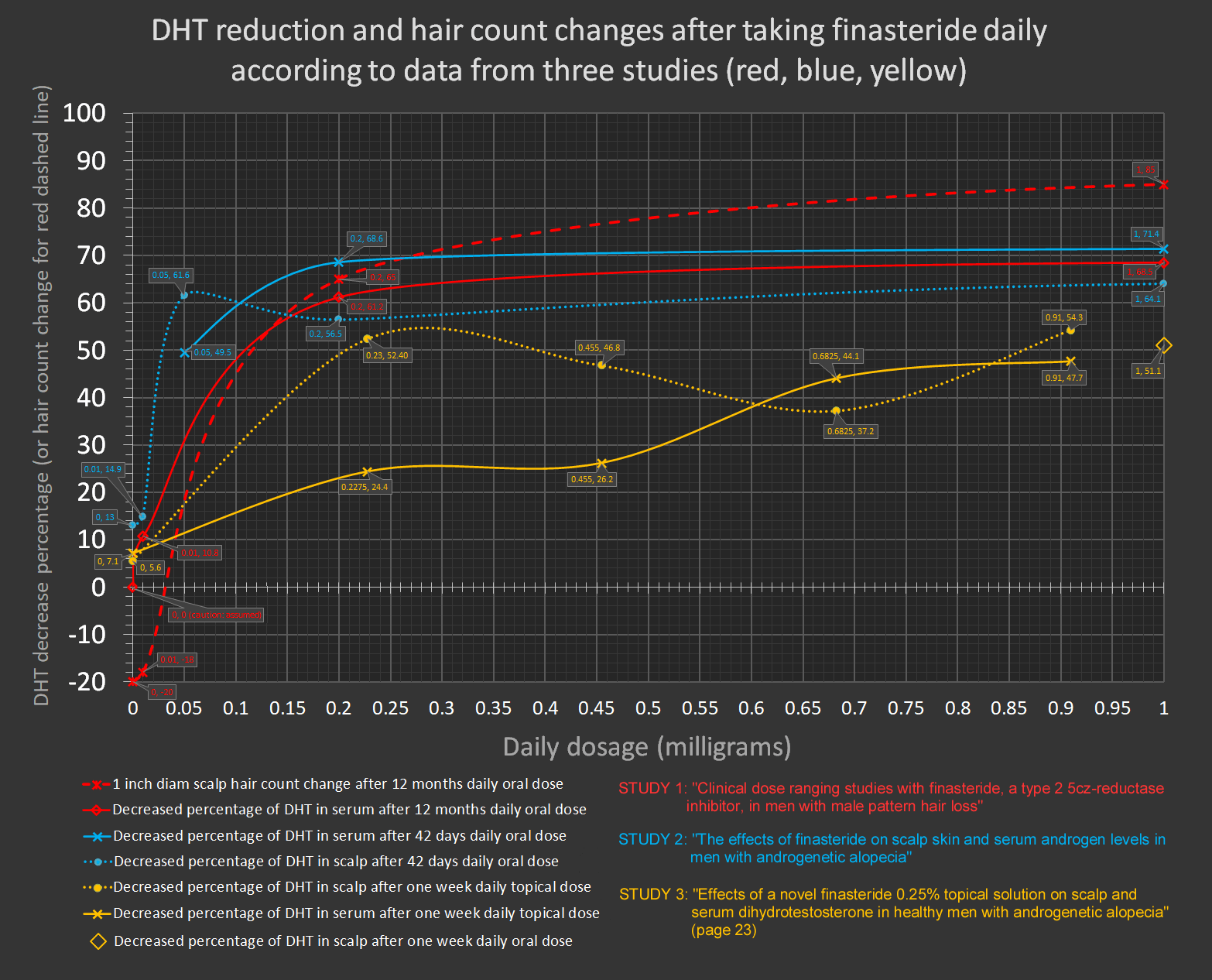
Study 1, Study 2, Study 3
And yet, that level is not zero! Where is that remaining DHT coming from? Well, the details get slightly more complicated than the story so far.
5α-reductase comes in three similar flavors or “isoenzymes”, types I, II, and III. Type I is all over the body, Type II is concentrated in androgen-responsive organs and male/female reproductive tracts, and Type III is even-more-everywhere than Type I (but mostly performs a different function and only weakly performs 5a-reductase activity.) finasteride mostly targets Type II, and weakly targets Type III, but mostly does not touch Type I. This is fine for hair loss, since it’s Type II which is responsible for most of the testosterone->DHT pipeline.
Unfortunately, for our present purposes of curing PMS/PMDD it’s Type I which is the main contributor to ALLO production in the brain where Type II is absent; exactly the weak-spot of finasteride. Which brings us to…
Dutasteride
Dutasteride is a potent inhibitor of both Type I, and Type II isoenzymes of 5-AR. (And, as a bonus, also inhibits Type III.) On dutasteride, DHT levels fall to less than 5-10% of the unmedicated concentration.[6] Since this 5-AR inhibitor knocks out what ought to be the most important isoenzyme of 5-AR for ALLO production, it’s of special interest to those of us who wish to cure PMS/PMDD.
I am not the first to realize all of this. In 2015, there was a study describing the administration of high-dosage (2.5mg/day for a month) dutasteride for the treatment of PMDD! As the model developed in this post predicts, the women in the study receiving the treatment reported significant reduction in anxiety, irritability, and sadness relative to controls. (N.B. The study was small. 16 people, 8 in each group.)
…Unfortunately the half-life of dutasteride is very long. (4-5 weeks.) Which means that to get serum levels up to the amounts which were significant in that one study, you’d have to be on it throughout the follicular phase as well.[7]
That might be fine! (So long as you don’t get pregnant. See the last section for more.) But it also has more side-effect-surface-area than a drug that’s out of the system within a few days, so it is undesirable in principle.
Results So Far
Which is why we started with finasteride, 2.5mg / day starting around ovulation and through to menses. We did it last month and are in the middle of the luteal phase of this month, and so far results seem pretty fucking awesome. Certainly better than any other intervention we’ve tried! We aren’t doing much in the way of quantitative measurement of the changes, but qualitatively the effect was impossible to miss last month. There was a pretty rough day or two in the luteal phase last month…but that is insanely good relative to baseline. Usually we get a string of 7-14 very rough days.
I’m somewhat surprised by, and suspicious of, how well it worked, given the lack of Type I 5-AR inhibition, and given the null result of the study that used the more potent 5-AR inhibitor. I’m not really sure what to make of that. One way it could be working, I guess, is if a significant proportion of ALLO in the brain is imported from serum ALLO, making Type II 5-AR (the kind finasteride hits hard) relatively more important than I expected? But I have no idea if that’s true. Or maybe it was a fluke and it won’t work this month. …Or…cue lightning and creepy organ music…maybe there’s some finicky threshold of ALLO concentration which switches the paradoxical response into the typical response and the finasteride brings it down below that threshold…shiver. (But then the PMS at the end of the cycle should still happen, right? And it didn’t last month.)
Regardless, whether it is obviously working or not this month there’s a good chance we’ll try dutasteride next month and I intend to report back in and edit to the end of this post if so.
Come ON ALREADY
Imagine all this is basically correct. 5-AR inhibitors work to fix PMS/PMDD because they stop the rise of allopregnanolone, and preventing the rise of ALLO works to fix PMS/PMDD because of how ALLO interacts with receptors. Even better than a 5-AR inhibitor, then, in terms of expected effectiveness and lack of side-effects, would be something that just blocked ALLO’s effects on receptors. Ah if only…
Wait a damn minute. “Isoallopregnanolone” does exactly that. And it was developed as a drug called “Sepranolone” back in 2010. But then…nothing? It looks like it got to “Phase II” trials but then either the company (“Asarina Pharma”) went under or lost interest or couldn’t show it did what they wanted it to do, or something I don't know what. It was purchased by “Relmada” in Feb of this year and it looks like they are trying to get it used as a Tourette syndrome treatment.
…So, keep an eye on that I guess.
iM nOt A dOcToR
But really, I have hardly touched on anything like potential side effects, and even though I’ll mention some things here you should definitely assume that I am missing something and go check it out yourself before feeding yourself or your partner a 5-AR inhibitor.
Number one thing: Do not take 5-AR inhibitors if you are going to get pregnant. Standard advice is not to even handle dutasteride if you are pregnant. 5-AR is extremely important to fetal development.
Lesser concerns: I haven’t looked very deeply into these claims, but Wikipedia tells me that 2% of men on finasteride get some amount of depression. A more significant fraction of men on finasteride (5%? 15%?) might get some kind of sexual side effect like low libido. (Though mechanically, finasteride ought to at least temporarily increase testosterone at least somewhat while it decreases DHT since the former is metabolized into the latter. And as that might make you think, when I started taking finasteride I found my libido to rise rather than fall and it subjectively seems to have remained at least as high as it was prior to the drug.) For women…I don’t know. That one study that gave women dutasteride found no ill effects (and for the women with PMDD, they saw increased libido) ….but that study only had 16 people in it so take that for what it is.
Another reason to start with finasteride, despite the stronger case for dutasteride in terms of the mechanism of action, is that finasteride has a much shorter half-life. If anything seemed to be going wrong, we could just stop the medication and within a few days it should be flushed from the system.
There are probably other possible problems with inhibiting 5-AR, but heuristically many men are on these inhibitors long term and are just fine, and I don’t immediately see why that should be different for women especially given the happy result of that dutasteride study. But, uh, do your own research, as they say.
- ^
These seem to be the same thing, differing only by whether the patient has an existing diagnosis for depression/anxiety apart from the luteal-phase woes. I’m just going to refer to both diagnoses as “PMDD” for the purposes of this post.
- ^
Aside from the compelling mechanism described below which progesterone fits into, further reasons to think it’s progesterone and not estrogen causing luteal-blues are: 1) Estrogen spikes even higher than this prior to ovulation, and this is typically regarded as an especially good time to have a uterus, and 2) “the implant,” Nexplanon, an implantable form of birth control that lasts around 3 years, seems to have a fair bit of anecdotal accounts of women getting a spike in depression and anxiety while under its effect. The hormone it releases as its mechanism of action? Progesterone (well, a synthetic version.) Of personal interest, my girlfriend tried the implant many years ago and spent the following ~year lightly menstruating constantly, and in the worst depression of her life. When she took it out, the effects cleared up. Together, these things start painting a pretty clear picture.
- ^
- ^
I had grown up thinking that all treatments for male baldness were always snake-oil, indeed I pictured hair-loss cures as the prototypical example of “snake-oil”. As it turns out, there are exactly 2 interventions which actually seem to work for a lot of men! If you’re a guy going bald, especially if you’re catching it early, getting on a 5α-reductase inhibitor and topical minoxidil has a good chance of stopping and maybe reversing the balding process. See the section on warnings/side-effects though. (tl;dr, they seem like a real thing to track but way overblown online.)
- ^
5α-reductase does a handful of other things too but, at least at the levels of inhibition which are achieved by long term use of hair-loss drugs, can’t be very reliably disruptive since lots of men are on them and doing just fine, and afaict the only women-specific 5α-reductase dependent pathways are mega ALLO production and various developmental purposes for growing babies. More on that in the warnings section at the end.
- ^
Why not 0% if it’s hitting all three of the 5-AR isoenzymes? IIUC, there are other ways the body produces small amounts of DHT, and also dutasteride may not be as potent an inhibitor of Type III.
- ^
Or take a mega-dose, I guess, but please don’t do that without researching whether or not that’ll kill you. Also you’ll end up with a bunch of dutasteride in your system throughout the follicular phase regardless, over time, if you take any amount even as infrequently as once a month.
Discuss
